Why Vision Care Should Be Part of the Health Equity Conversation
Preventable vision loss does not occur at random. Across income levels, racial groups, and geographic regions, the burden of avoidable blindness and visual impairment falls heaviest on communities that already face compounding health disparities, making eye care an inseparable part of the broader health equity conversation.
Vision is directly tied to outcomes that extend well beyond the clinic. Children with uncorrected refractive errors fall behind in school. Adults with untreated eye disease face reduced employment prospects and diminished independence. For people managing chronic conditions like diabetes, access to regular eye examinations is a functional necessity, not an optional service.
Despite this, vision care has long remained on the margins of health equity policy. When it is excluded from equity frameworks, a significant and measurable source of avoidable harm goes unaddressed. Recognizing the role that health inequities play in shaping who loses sight, and who receives timely care, is the first step toward integrating eye health into the policy conversations where it has always belonged.
Why Vision Care Belongs in Health Equity
Preventable vision loss tracks closely with broader patterns of health inequities. The communities most affected by avoidable blindness are, in most cases, the same communities already navigating compounding disadvantages in housing, income, and healthcare access. This is not coincidental; it reflects how structural conditions shape health outcomes across every domain, including eye health.
Eye care connects directly to education, employment, chronic disease management, mobility, and quality of life. When vision needs go unmet, the consequences ripple outward in ways that are both measurable and preventable. Excluding vision care from equity policy, therefore, leaves a major source of avoidable harm unaddressed and weakens the overall framework designed to close health disparities.
How Inequity Shapes Eye Health Outcomes
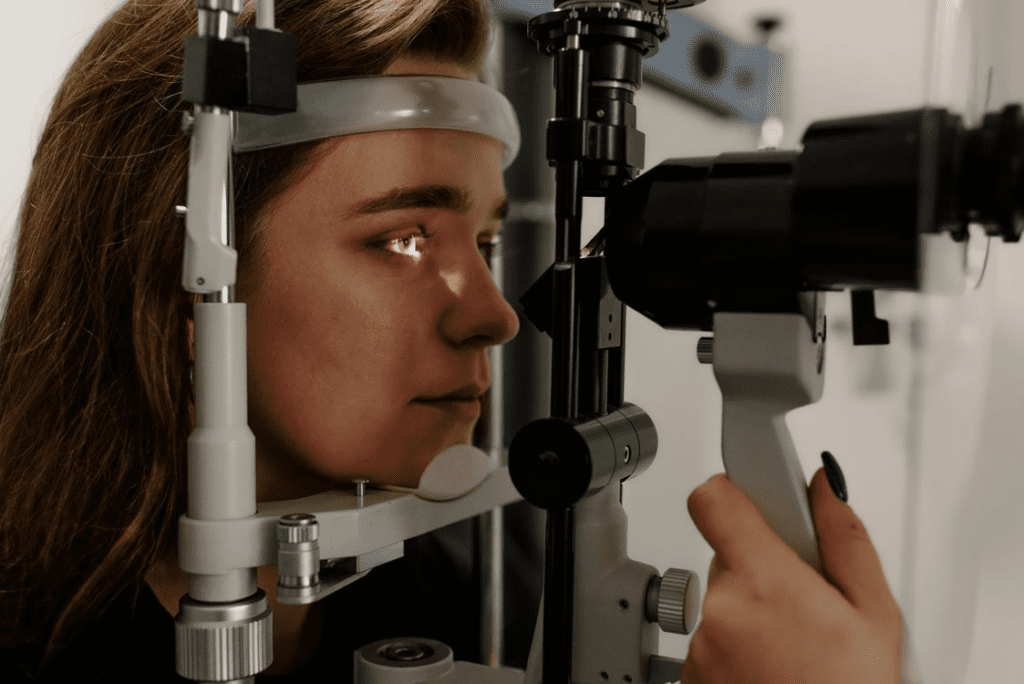
Access to vision care spans routine screening, chronic disease management, and informed evaluation of treatment pathways when clinically appropriate. Yet for many patients, that access is shaped less by clinical need than by social circumstance. Understanding how inequity produces unequal eye health outcomes requires looking at both the structural conditions that limit care and the clinical consequences that follow when care is delayed.
For patients who do reach the point of evaluating their options, questions such as is refractive lens exchange right for you reflect the kind of informed decision-making that depends on consistent, accessible care navigation, something many underserved patients never have the opportunity to engage with.
Social Conditions That Limit Access to Care
The social determinants of health, which include income, insurance status, transportation, geography, and health literacy, directly shape whether a person receives timely eye care or goes without it for years.
For many in underserved populations, the barriers compound quickly. Without insurance, a routine eye exam becomes an out-of-pocket cost that competes with rent or food. Without reliable transportation, a specialist appointment in a neighboring county may as well be unreachable.
Health literacy adds another layer. When a patient does not fully understand a diagnosis or follow-up instructions, the likelihood of returning for care drops significantly. These are structural conditions, not individual failures, and they produce predictable gaps in who receives care and who does not.
Why Some Eye Diseases Go Untreated Longer
Racial disparities and socioeconomic status are consistently associated with delayed screening and interrupted follow-up, a pattern documented in government data from the CDC.
Diabetic retinopathy and glaucoma illustrate the consequences clearly. Both conditions progress silently in early stages, which means regular monitoring is the only reliable safeguard. Patients who lack consistent eye care access in underserved communities often present with advanced disease, at which point treatment options narrow considerably.
Who Is Most Affected by Vision Disparities

The communities carrying the heaviest burden of vision loss are well documented. Research from the National Eye Institute and population-level surveillance data consistently identify Black, Hispanic, low-income, and uninsured individuals as facing disproportionate rates of avoidable visual impairment.
Older adults represent another high-burden group, as age-related conditions like glaucoma and macular degeneration require sustained access to care that many cannot maintain. When income constraints, insurance gaps, and mobility limitations converge, the risk of undetected disease rises considerably.
Geographic location further compounds these health disparities. Rural communities and federally designated healthcare shortage areas have fewer practicing optometrists and ophthalmologists per capita, meaning residents often travel significant distances for care they may ultimately defer or forgo entirely.
Critically, these patterns do not begin in adulthood. Pediatric screening gaps mean that children in underserved populations frequently enter school with uncorrected vision problems that go unidentified for years, and racial disparities in childhood screening rates suggest the inequity is established well before chronic eye disease becomes the primary concern.
What Untreated Vision Needs Cost Communities
The downstream effects of untreated vision conditions extend well beyond the eye clinic. Children with unaddressed refractive errors struggle to keep pace academically, adults with progressive eye disease face narrowing employment options, and older individuals lose the independence that intact vision supports. For those managing diabetes or hypertension, skipped eye appointments also mean missed opportunities to monitor systemic disease progression.
Delayed eye care carries real financial consequences as well. When conditions like glaucoma or diabetic retinopathy are identified late, treatment becomes more intensive and more expensive, shifting costs onto patients, families, and health systems simultaneously. Medicare and Medicaid bear a disproportionate share of these downstream expenditures, particularly as preventable vision loss accelerates the need for disability support and assisted living services.
This is why preventing vision impairment before it starts belongs at the center of any equity strategy, not at its margins. Framing early intervention and consistent access to eye care as optional underestimates how deeply vision loss interacts with the social determinants of health, and how significantly health inequities compound when basic visual needs go unmet across entire communities.
What Would Make Vision Care More Equitable
The barriers described throughout this article, from coverage gaps and workforce shortages to delayed diagnoses and pediatric screening failures, are not inevitable. They reflect policy choices that can be revisited. Meaningful reform requires action on both the financing side and the delivery side of care.
Coverage and Workforce Changes
Meaningful progress on vision equity begins with coverage. Expanding Medicaid to include routine and specialty eye services would bring preventive care within reach for millions of low-income adults who currently go without it. Medicare coverage gaps for standard eye exams remain a well-documented barrier for older populations, and closing them would directly reduce delayed diagnoses.
Workforce distribution matters equally. Shortage areas need expanded referral pathways that connect primary care providers to ophthalmology and optometry networks. Culturally responsive care, including language access and community-based outreach, improves both engagement and follow-through in populations with historically low retention in eye care.
Screening, Data, and Teleophthalmology
Teleophthalmology has emerged as a scalable mechanism for reaching patients in geographically isolated communities, enabling diabetic retinopathy screening and early detection without requiring specialist proximity. The American Academy of Ophthalmology has highlighted remote imaging programs as a practical tool for narrowing access-to-care disparities.
Better disparity data remains foundational to any health equity strategy. Without disaggregated screening and outcomes data, identifying where gaps persist, and measuring whether interventions are working, is not reliably possible.
Why This Conversation Cannot Leave Vision Behind
Health equity frameworks that overlook vision care leave a measurable gap in both policy and practice. The evidence reviewed across access, outcomes, and community burden points consistently in one direction: vision loss follows the same structural fault lines as other preventable health disparities, and it demands the same level of policy attention.
Eye care is not a peripheral concern. When coverage gaps, workforce shortages, and screening failures converge, vision loss compounds inequality across education, employment, and aging. Addressing these conditions is a shared policy responsibility, and the frameworks designed to advance health equity are stronger when eye health is built into them from the start.